Trauma-Informed Leadership in Healthcare: Why Understanding Ourselves Matters for Patient Safety
Introduction
Over the last year, I have been quieter than usual on LinkedIn and social media.
It wasn't because I had lost interest in healthcare, governance, patient safety, or leadership. Quite the opposite.
I was doing something I should probably have done years ago.
I was working on myself.
Like many people working in healthcare, I spent years focusing on everyone else's needs. Patients. Staff. Organisations. Services. Improvement projects. Regulatory requirements. Governance systems. Risk registers. Incident investigations.
What I rarely stopped to consider was how my own experiences, beliefs, coping mechanisms, and unresolved trauma influenced the way I led.
Through therapy and self-reflection, I began to understand something that has fundamentally changed how I view leadership.
The systems we build are often a reflection of the people leading them.
And if we want safer organisations, stronger cultures, and better patient outcomes, we need to be willing to look beyond policies and procedures and explore the human beings behind them.
The Leadership Conversation We Rarely Have
Healthcare leadership is often discussed in terms of strategy, governance, performance, finance, and regulation.
We talk about:
- Staffing shortages
- Quality indicators
- Patient safety metrics
- Inspection outcomes
- Workforce challenges
- Organisational performance
All of these things matter.
But there is a question we rarely ask:
Who are the people leading these systems?
Every leader arrives with a lifetime of experiences.
Some arrive having grown up in stable environments where they learned trust, confidence, and emotional security.
Others arrive carrying experiences of adversity, trauma, neglect, instability, loss, or chronic stress.
Those experiences do not disappear when we step into leadership roles.
They influence how we communicate, how we manage conflict, how we respond to pressure, and how we make decisions.
In healthcare, where decisions can affect patient outcomes, this matters more than we often realise.
Trauma Doesn't Stay at Home
When people hear the word trauma, they often think of major life events.
But trauma is not defined solely by what happened to us.
It is often defined by how our nervous system learned to adapt in order to survive.
Many of the traits that help people become successful healthcare leaders can also be rooted in coping mechanisms developed much earlier in life.
For example:
Hyper-Responsibility
Many healthcare leaders carry an overwhelming sense of responsibility.
They struggle to switch off.
They feel personally accountable for everything.
They take on too much and find it difficult to ask for help.
On the surface, this can look like commitment.But beneath it may be a deeply ingrained belief that they must hold everything together because nobody else will.
Perfectionism
Healthcare attracts perfectionists.
Attention to detail is important.
But perfectionism can also create fear.
Fear of failure.
Fear of criticism.
Fear of making mistakes.
When leaders cannot tolerate imperfection in themselves, they often struggle to tolerate it in others.This can undermine learning cultures and psychological safety.
Avoidance
Some leaders avoid difficult conversations.
Others delay decisions.
Others become overwhelmed by conflict.
These responses are rarely about capability.
They are often about emotional survival strategies developed long before leadership positions were ever considered.
Control
Many leaders find delegation difficult.
They feel safer when they maintain direct oversight.
The challenge is that organisations become dependent on them, teams lose autonomy, and growth becomes limited.
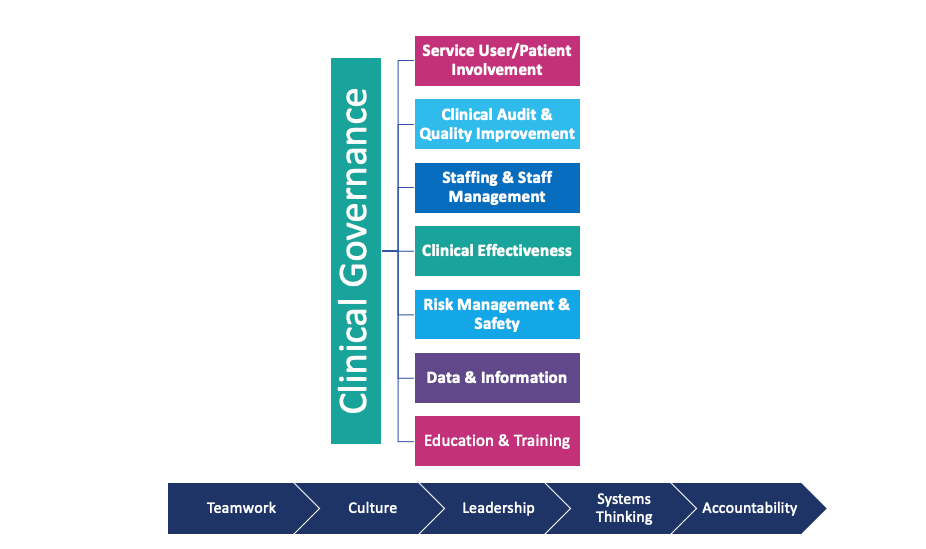
What Does This Have to Do With Patient Safety?
Everything.
Patient safety is often viewed through the lens of systems, processes, and governance.
Those things are essential.
But patient safety is also influenced by culture.
And culture is heavily influenced by leadership.
Consider the following:
Psychological Safety
If staff fear criticism, blame, or humiliation, they are less likely to speak up.
Concerns remain hidden.
Near misses go unreported.
Learning opportunities are lost.
Incident Reporting
If leaders react defensively when incidents occur, staff quickly learn that reporting is risky.
The result is under-reporting, reduced transparency, and missed opportunities for improvement.
Duty of Candour
Being open about mistakes requires emotional maturity and self-awareness.
Leaders who struggle with shame or fear may unintentionally create environments where openness becomes difficult.
Risk Management
Leaders who avoid discomfort may avoid difficult risks.
Leaders who fear conflict may tolerate poor performance.
Leaders who need control may struggle to empower others.
These behaviours can directly affect organisational safety.
What Therapy Taught Me About Governance
For much of my career, I believed good governance was primarily about systems.
Risk registers.
Policies.
Audits.
Committees.
Performance reports.
These things remain important.
But what I have learned is that governance is also about people.
You can have the best policies in the world.
You can have comprehensive audits.
You can have sophisticated reporting systems.
But if leaders are unable to receive challenge, admit mistakes, or create psychological safety, governance will always be limited.
The most effective governance systems are supported by leaders who are willing to reflect on themselves.
Leaders who understand their strengths.
Leaders who recognise their triggers.
Leaders who are curious about their own behaviours.
Leaders who understand that self-awareness is not a weakness but a governance asset.
Trauma-Informed Leadership Is Not Soft Leadership
This is one of the biggest misconceptions.
Trauma-informed leadership is often misunderstood as being less accountable or less demanding.
In reality, the opposite is true.
Trauma-informed leaders still:
- Hold people accountable
- Address performance concerns
- Make difficult decisions
- Manage risk
- Maintain standards
The difference is how they do it.
They understand that people perform best when they feel psychologically safe.
They recognise that curiosity often produces better outcomes than judgement.
They understand that learning is more powerful than blame.
And they appreciate that culture is built through everyday interactions rather than policies alone.
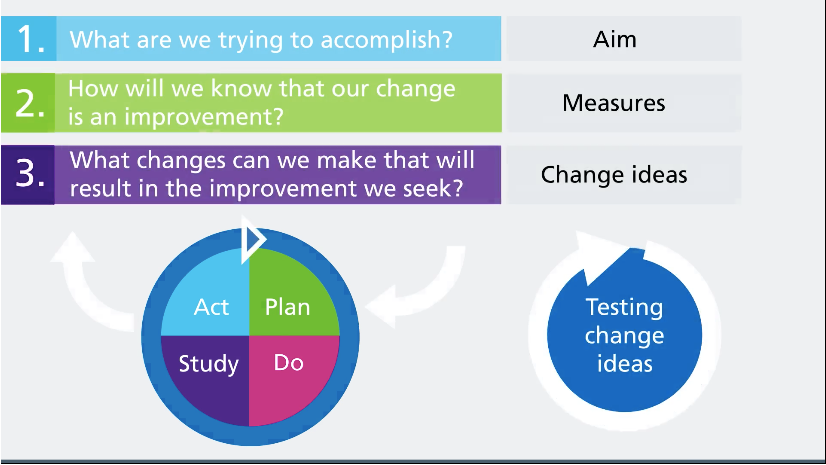
Building Trauma-Informed Healthcare Organisations
Trauma-informed leadership is not simply about individual leaders.
It also influences how organisations operate.
Healthcare organisations can become more trauma-informed by:
Creating Psychological Safety
Encouraging staff to speak openly about concerns, incidents, and mistakes without fear.
Supporting Reflective Practice
Giving staff and leaders opportunities to learn from experiences.
Moving Beyond Blame
Focusing on systems and contributing factors rather than individual fault.
Investing in Leadership Development
Developing emotional intelligence alongside technical and operational skills.
Prioritising Wellbeing
Recognising that workforce wellbeing and patient safety are closely connected.
The Future of Healthcare Leadership
Healthcare is becoming increasingly complex.
Leaders face unprecedented pressures.
Financial challenges.
Regulatory scrutiny.
Workforce shortages.
Growing patient demand.
Traditional leadership models focused solely on performance and compliance are no longer enough.
The healthcare leaders of the future will need:
- Governance expertise
- Patient safety knowledge
- Emotional intelligence
- Self-awareness
- Systems thinking
- Compassionate leadership skills
These are not competing priorities.
They are complementary capabilities.
The strongest leaders will be those who understand both organisations and themselves.
Conclusion
Over the last year, I have learned that leadership is not just about understanding organisations.
It is also about understanding ourselves.
- The systems we create.
- The cultures we build.
- The decisions we make.
- The way we respond to challenge.
- The way we treat people.
All of these things are influenced by the stories we carry.
As healthcare leaders, we spend considerable time asking organisations to learn from incidents.
Perhaps we should spend more time learning from ourselves too.
Because one of the most important patient safety interventions we can make may not be a new policy, audit programme, or governance framework.
It may be the willingness to look inward, understand our own experiences, and lead with greater awareness, compassion, and authenticity.
In doing so, we create safer environments not only for our staff, but ultimately for the patients who depend on us.
Email Us
For general enquiries & questions,
contact us via email
Book Free Consultation
Need some advice face to face? Book a free 30 minute MS Teams consultation
Share
CHECK OUT OUR OTHER BLOG POSTS
Healthcare Insights